Wei Zhang1,
Hui-Ming Yi1,
Xi Ai2,
Kai-Yan Li1,
You-Bin Deng1 ![]()
For correspondence:- You-Bin Deng Email: docdengyb@163.com Tel:+862783663554
Received: 1 July 2015 Accepted: 1 March 2016 Published: 30 April 2016
Citation: Zhang W, Yi H, Ai X, Li K, Deng Y. Analysis of only 0-1 min clip or 1-4 min Clip for focal liver lesions during contrast-enhanced ultrasonography. Trop J Pharm Res 2016; 15(4):833-839 doi: 10.4314/tjpr.v15i4.24
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To evaluate the reliability of analysis of only 0-1min clips and 1-4min clips versus the entire clips in performing contrast-enhanced ultrasonography (CEUS) of focal liver lesions (FLLs).
Methods: Contrast-enhanced ultrasonography (CEUS) examinations of 43 single FLLs were performed. All clips were analyzed in three ways, the entire clips, 0-1 min clips and 1-4 min clips, benign or malignant diagnosis and pathological diagnosis of each FLL were concluded by the three ways subsequently.
Results: The results of correct diagnosis were assessed using Chi-square test. There was no difference with regard to benign or malignant diagnosis, between 0-1min clips and the entire clips, or between 1-4 min clips and the entire clips (p = 0.243 and p = 0.747, respectively). Moreover, no significant differences in pathological diagnosis existed between 0-1min clips and the entire clips, and 1-4min clips versus entire clips (p=0.808 and p = 0.808, respectively). No significant differences existed among CEUS entire clip, 0-1min clip and 1-4min clip in identifying FLLs, and based on which the diagnosis of two different FLLs during CEUS with only one injection of contrast agent can be available.
Conclusion:Only 0-1min clips or 1-4 min clips can be used to instead of the entre clip in performing CEUS of FLLs.
Introduction
Contrast-enhanced ultrasonography (CEUS) is a widespread imaging procedure for investigating the liver parenchyma. The injection of ultrasound contrast agents (USCA) and the use of specialized imaging techniques now allow to display tissue macro and micro-vascularization similarly to what is seen with contrast- enhanced computed tomography (CECT) or magnetic resonance imaging (CEMRI) [1]. Ultrasound contrast agents present a pure intravascular distribution and do not leak in the interstitial space but persist in the sinusoids and portal vessels without the evidence of any equilibrium phase [2]. The peculiar hepatic vascularization allows defining different vascular phases. The arterial phase starts from 10-20 s after the injection of MBs, lasts for approximately 10 - 15 s and provides information on the degree and pattern of vascularity. The portal phase then lasts for 2 min after the start of injection, whereas the subsequent late phase lasts for up to 4–6 min after injection, until microbubble clearance from the liver parenchyma. Both portal phase and late phase provide information about the wash-out of focal liver lesions (FLLs) compared to the surrounding parenchyma (the term wash-out describes a transition from some enhancement of a lesion, either iso- or hyper enhancement, to a clear hypoenhancement) [3].
During the last few years, many studies have investigated the CEUS patterns of FLLs, establishing their typical behavior in the arterial, portal and venous phases [3]. Several papers have described the general capabilities of CEUS in improving focal liver lesion characterization [2]. CEUS is now a reliable imaging tool with well-established applications in the characterization of liver lesions with the possibility of prolonged liver ultrasound examination, and is easily performed.
One limitation of CEUS in comparison to multiphase CT and MR imaging is the fact that only one liver lesion can be examined at a time as the transducer has to be kept still during the examination, and further contrast injections are necessary to characterize additional liver tumors.
To date, a single clip over 180 s is required to analyze all phases (arterial, venous and late phases) of contrast behavior. The process lasts a long time and thus has to be performed off-line in “back-office” work and the analysis of entire video clips is very time-consuming and demanding in terms of technical resources, thus limiting potential applications in routine clinical use especially in assessing two different FLLs. In the attempt to simplify the process and to reduces acquisition time associated with CEUS, the entire clips of CEUS were divided into two clips, 0-1min clips and 1-4min clips, then the ratio of correct diagnosis and the statistical differences were analyzed in this study to evaluate the reliability of analysis of only 0-1min clips and 1-4min clips versus the entire clips.
Methods
Patients and lesions
All patients with single FLL who had undergone pathological examination originating from operation or biopsy and previously assessed with CEUS were considered eligible for this study. Patients with any of the following conditions were excluded:
1. Previous adverse reactions to Sonovue (Bracco Imaging, Milan, Italy),
2. Severe pulmonary hypertension;
3. Pregnancy or breastfeeding conditions;
4. Portal vein thrombus and postcava thrombus;
5. Evidence of critical illness or medical instability;
6. History of operation and minimally invasive therapy;
7. Poor image quality of the FLL.
Written informed consent was obtained from all patients before the examination, and the study was approved by the Institutional Review Board and Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (no. TJ-C20121213). All CEUS studies were performed for clinical purposes and were not performed merely for the purpose of the current study.
Imaging protocol
Vivid E9 (GE, America) equipped with a 3.5 MHz harmonic-imaging transducer was used for CEUS and clip recording. Initially, a B-mode scan was performed to identify the best approach to the lesion. This consisted in choosing a scan in which the lesion was located in the mid-near field and remained visible during respiratory movements. The choice of the mid-near field was made based on previous findings, showing that this region provides the highest reproducibility. Thereafter, a bolus of 2.4 ml of Sonovue (Bracco Imaging, Milan, Italy), a second generation contrast agent composed of microbubbles of sulphur hexafluoride, was injected intravenously in an antecubital vein with a 22-gauge angiocatheter, extension tubing and a three-way stopcock., followed by 5 ml flush of NaCl (0.9 %) in bolus. Zero time was recorded at the completion of Sonovue flush. A continuous video clip of CEUS was acquired (duration 3-4min) following contrast injection. All investigations were performed in the same standardized way by the same expert operator, with 10 years of experience in CEUS.
Imaging analysis
The CEUS clips were analyzed in 3 ways: (a) the entire clips, (b) 0-1min clips, referred to here as artery and earlier portal phase methodology, (c) 1-4min clips, referred to here as later portal phase and late phase methodology. The CEUS clips were divided by an external operator, following a training period.
All images, including grayscale, color Doppler ultrasound images and CEUS clips were evaluated in DICOM format with computer workstation. Two blinded radiologist readers, both with 5 years of experience in CEUS, independently reviewed all the ultrasound examinations. Both readers were blinded to clinical features, laboratory examinations and other imaging findings. Then readers were asked to provide the most likely diagnosis (i.e., benign or malignant diagnosis, pathological diagnosis or indeterminate) for each focal liver lesion according to standard diagnostic criteria [3,4].
Statistical analysis
Collected data were entered into a common spreadsheet and summary statistics were calculated. Categorical variables were assessed using the chi-square test. All the data were analyzed with SPSS 18.0. The results are expressed as mean ± standard deviation (SD) for each measurement. P < 0.05 was considered statistically significant.
Results
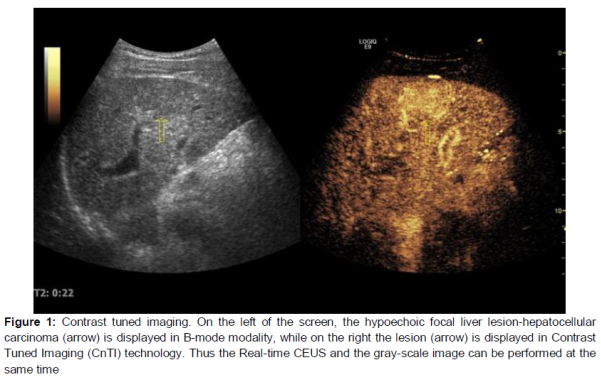
Contrast Tuned Imaging software was utilized for contrast detection (); dynamic range set at 7, mechanical index at 0.03, acoustic power at 40 kPa, frame rate at 15 Hz, sectorial gains at zero. Visualization was always kept in dual mode display.
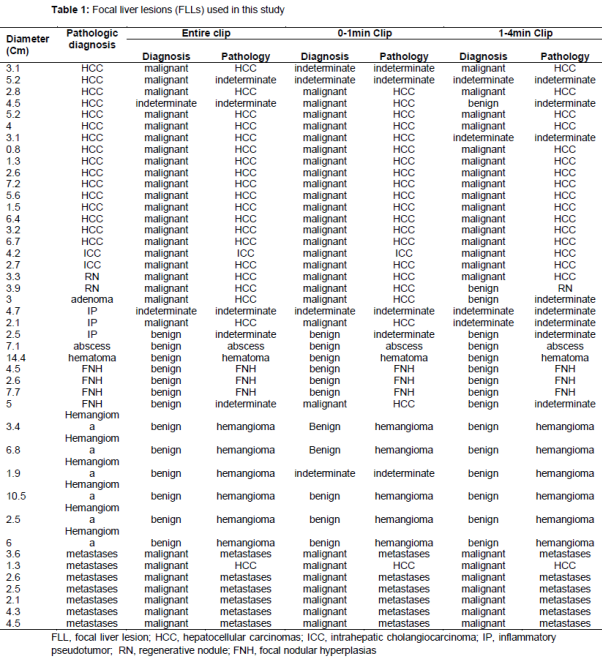
In our present investigation, 43 patients including 29 men and 14 women, who ranged in age from 21 to 78 years, with satisfactory image quality were analyzed. The differences in the clinical characteristics are reported in . The study comprised 43 lesions (16 hepatocellular carcinomas, 2 intrahepatic cholangiocarcinomas, 2 regenerative nodules, 7 liver metastases carcinomas, 4 focal nodular hyperplasias, 6hemangiomas, 1 hepatocellular adenoma, 3 inflammatory pseudotumors, 1 liver abscess, 1 hematoma). The final diagnosis was established using operation and biopsy. The median diameter of the lesions was 4.2 cm (0.8–14.4 cm).
The results of the entire clips, 0-1 min clips and 1-4 min clips concerning benign and malignant diagnosis as well as pathological diagnosis are shown in Tables 2 and 3. There were no differences with regard to benign or malignant diagnosis between 0-1min clips versus the entire clips as well as 1-4 min clips versus the entire clips (p = 0.243 and p = 0.747, respectively) (). Moreover, no significant differences in pathological diagnosis existed between 0-1 min clips versus the entire clips and 1-4 min clips versus the entire clips (p = 0.808 and p = 0.808, respectively) ().
Discussion
So far, many studies have investigated the CEUS patterns for FLLs examination, establishing their typical behavior in the arterial, portal and venous phases [3]. Malignancies typically show low echo-signal intensity at late phase [5,6], and the contrast pattern that characterizes benign FLLs is the absence of wash-out in the portal-venous and late phases [2]. Besides, benign and malignant FLLs may occur in cirrhosis and fatty liver [7,8].
To simplify the process and reduce the CEUS time, 0-1min clips and 1-4min clips were divided from entire clips in this study. Subsequently, no significant differences was found between 0-1min or 1-4min clips versus the entire clips with respect to malignant or benign diagnosis and pathological diagnosis, which means that 0-1min clip and 1-4min clip can be used independently to reach valid diagnosis in CEUS of FLLs. Additionally, our study also demonstrated that it’s possibility of CEUS for testing two different FLLs based on 0-1min and 1-4min clip with only one injection of contrast agent.
Typical haemangiomas will show peripheral nodular enhancement (PNE) in arterial phase of CEUS, whereas untypical haemangiomas would not observe PNE (especially seen in small haemangiomas), resulting in misdiagnosis by 0-1min clips, but the gray-scale ultrasound of hyperecho in normal liver tissue would help to obtain correct diagnosis [6,9,10]. In our study, for the 6 haemangiomapatients, 0-1min clips obtained correct pathologic diagnosis in 5 patients, and 1-4min and the entire clips obtained correct pathologic diagnosis in all the 6 patients. The CEUS characteristic of typical FNH is centrifugal filling with central spoke wheel-shaped contrast enhancement during the arterial phase [6,9,10]. Thus the absence of central spoke wheel may result in wrong diagnosis within FNH nodules, which might be misdiagnosed as malignant lesions because of rapidly filling in the artery phase. However, it did not affect the diagnosis as benign nodules by the entire clips and 1-4min clips in our investigation.
The HCC multistep carcinogenesis could lead to changes in intra-nodular blood supply, consisting in a progressive decrease of the portal supply associated to a decrease in normal arterial supply, subsequently overcome by increase of newly formed tumoral arterial supply [11-13]. Generally, regenerative nodules are nearly iso-enhancing in all phases but the not negligible rate of HCCs showing this same vascular pattern (the so-called “hypovascular HCC” approximately 10-20 %) [14]. The differential diagnosis among regenerative nodule, hepatocellular adenoma and HCC is not always easy to be reached, which imposes a strict recall strategy for any newly detected lesion in cirrhosis [15]. Contrast features of metastases at CEUS are hyper-enhancement during the arterial phase (or rim-like enhancement with non-enhancing central areas in hypo-vascular metastases) followed by marked hypo-enhancement during the late phase [16]. Metastases especially small FLL, without hypo-enhancement, present homogenous enhancement, may influence the diagnosis by the entire clip and 0-1min clip. But the history and appearance of multiply FLLs can do some help. Intrahepatic cholangiocarcinoma (ICC) is a tough diagnostic challenge duo to its asymptomatic clinical features and atypical imaging characteristics [17,18]. Commonly, it is more difficult to distinguish smaller ICC (diameter ≤3 cm) from HCC on CEUS, corresponding to more frequently appeared homogeneous hyper-enhancement [19]. In our study, similar with the entire clips, the 0-1min clips could correct diagnose 14 in 16 patients. In addition, for the 7 patients with liver metastases, all the 0-1min, 1-4 min and entire clips could correct diagnose 6 patients.
Inflammatory pseudotumor (IP) is an uncommon benign lesion with a variable degree of CEUS enhancement appearance [20]. In this study, one IP with absent contrast enhancement was diagnosed correctly, while two IPs with enhancement in arterial phase and hypoechoic appearance in late phases were misdiagnosed as HCC or indeterminate lesion. This phenomenon has been seen in another study [21]. The various CEUS patterns of IP were deemed to relate with different quantity of cellular areas and intense fibrosis areas [20,22]. Unfortunately, until now, there has been no systematic report on the CEUS appearance of IP, which needs further study. In routine clinical practice, a definitive and exact differential diagnosis of FLLs with CEUS entire clip is possible only in some types of lesions, whilst the simple categorization of a lesion as benign or malignant can be achieved with extremely high sensitivity (>90 %) and specificity [2], as well as with an accuracy comparable to CT or MRI in most series [23-26]. Additionally, in typical lesions the 0-1min clip and 1-4min clip could be comparable to the entire clip in diagnosis of FLLs aforementioned.
However, we could see that some lesions might have atypical contrast-enhancement patterns (ACEP), which may lead to misdiagnosis. Between 5 and 25 % FLLs remains indeterminate even after CEUS (especially in cirrhotic livers) [5,6,9,21,27,28]. These situations could go against the 0-1min clip and 1-4min clip derived from the entire CEUS clip much more seriously. Thus, the ACEP FLLs need to be characterized by other diagnostic investigations.
Limitations of the study
First, the main limitation of the study was that s other FLLs were not included in the study and some of them may be difficult to differentiate from each other [29,30]. Therefore, the results of the study are only applicable for FLLs mentioned above. Second, since the FLLs number in our study is limited, the usefulness of 0-1min clip and 1-4min clip in diagnosing FLLs is needed further investigation with large cases. Third, these findings might be related to the fact that both readers were blinded to the liver etiology history, elevation of serum biomarkers such as alpha-fetoprotein or CA, and other laboratory findings, as well as other imaging findings or clinical presentations. The authors believe that precise patient history and/or further examinations are mandatory to reach a correct differential diagnosis. In addition, the experiences of radiologists in CEUS will influence the diagnosis of FLL.
Conclusion
The findings of this study demonstrate that there is no significant difference between CEUS entire clip, 0-1min clip and 1-4 min clip in identifying FLLs, and based on which the diagnosis of two different FLLs during CEUS with only one injection of contrast agent can be available. The findings also demonstrate that the appearance of lesions in the arterial phase is also very important when distinguishing between benign and malignant lesions, although appearance in the portal and late phases is important when characterizing them.
References
Archives


News Updates